
Endometriosis, with its medical name, is a common health problem in women. In this article, you can find answers to all questions about the causes, symptoms, treatment and chocolate cyst (endometrioma) surgery of endometriosis disease, in which many factors play an important role.
The incidence of endometriosis is not known precisely. It is considered an important women's health problem because it impairs the patient's quality of life and may cause infertility,
The diagnosis of chocolate cyst (endometriosis) is definitively made with surgery. Its incidence in the population is estimated to be 10% in women of reproductive age and 25-35% in infertile women.
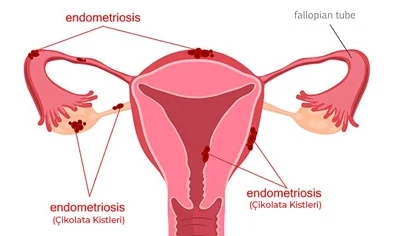
Endometriosis, colloquially, chocolate cyst disease, is the extrauterine location of glandular tissue (endometrium) that forms the inner part of the uterus and provides menstrual bleeding in normal physiology.
Where the inner membrane layer of the uterus (endometrium) is located, it holds the organ and causes complaints according to the organ it holds. Endometriosis can affect the ovaries, abdominal cavity, intestines, outer lining of the uterus, bladder, lungs, and even the brain.
If endometriosis occupies the ovary and causes a cyst, it is called an endometrioma, popularly known as a chocolate cyst.
It is not known exactly what causes endometriosis. Many theories have been put forward about how the chocolate cyst forms, but none of them has been clarified. Regardless of the theory, the underlying genetic predisposition is seen as the most important risk factor. Probably not the only theory, but the combination of these theories causes a chocolate cyst.
One of the most accepted theories is that the blood that needs to be thrown out during menstruation goes back to the tubes from the uterus and spreads from there to the abdominal cavity, intestines and ovaries. It is thought that the living endometrial cells in this blood settle in the organ where they go and continue to grow there.
The fact that endometriosis is more common in those with heavy menstrual bleeding, prolonged and frequent menstruation supports this theory.
However, studies have shown that almost all women bleed backwards, but chocolate cysts do not form in all of these women. For this reason, it is thought that the underlying genetic predisposition plays an important role in the development of chocolate cyst.
According to this theory, it is claimed that the epithelium in the organs that develop endometriosis undergoes self-change (metaplasia). However, the question of why this change does not occur in everyone cannot be answered.
The presence of endometriosis in the lungs and brain has been tried to be explained by blood and lymphatic spread, but no consensus has been reached on this issue either.
Lymph circulation is a circulatory pathway that continues outside of the intravascular circulation and is thought to play a role in the transport of endometriosis cells.
Perhaps the only consensus theory about how a chocolate cyst occurs is genetic predisposition. Because the incidence of endometriosis in the relatives of those with chocolate cysts was found to be much higher than in the normal population.
Decreased immune system is also counted among the causes of chocolate cyst. Even if there is a backward blood flow during menstruation, a woman with a normal immune system will destroy these endometrial cells that go out of the uterus by natural killer cells.
As a result, viable endometrial cells cannot survive in those areas and are destroyed. However, if the immune system is weak, endometriotic cells cannot be cleared by the body and continue to grow where they go.
One of the mechanisms that play a key role in the development of endometriosis is the increase in estrogen level as a result of increased aromatase enzyme activity. Chocolate cyst is actually an estrogen dependent disease. Endometriosis is not seen before puberty and after menopause (periods of low estrogen production in the body). This also supports this theory.
As cyclooxygenase 2 activity increases in women with chocolate cysts, prostaglandin production also increases. This causes painful menstruation and groin pain.
Apart from these, complaints such as waist, leg, back pain, difficulty in defecation, blood in the urine or stool may also be seen. If there is lung involvement, blood coming from the throat can also be seen when coughing. Patients with bladder involvement may experience pain during urination and blood in the urine.
Sometimes a chocolate cyst may not cause any symptoms. Chocolate cyst can be detected incidentally by ultrasound during routine examinations.
Chocolate cysts are more common in those with;
Chocolate cyst is mostly seen in women of reproductive age between the ages of 15-45. It is not seen before puberty and after menopause. Chocolate cyst is an estrogen dependent disease.
Since the body estrogen decreases before puberty and after menopause, it regresses even if there is a disease. In girls who have painful menstruation in adolescence, endometriosis may be encountered in 8-10 years in advancing ages.
Chocolate cyst is diagnosed based on the patient's symptoms. Chocolate cyst is suspected if one or more of the complaints of menstrual pain, pain in intercourse or inability to become pregnant are present.
Immobility of the uterus and the impression that the back of the uterus is adhered on examination suggests endometriosis. With transvaginal ultrasound examination, adherent bowel segments that continue on the posterior wall of the uterus can be detected.
Chocolate cyst can be diagnosed more easily with ultrasound. If the chocolate cyst has not formed, if there are only endometriotic focus, it may be difficult to detect with ultrasonography. The experience of the viewer influences the success of the examination. If there are deep focus, they can be diagnosed with MRI (Magnetic Resonance).
Chocolate cyst or early stage endometriosis may develop without causing any symptoms and may be detected incidentally during a gynecological examination or during surgery. Inguinal pain and advanced stage of the disease are not directly proportional.
The definitive diagnosis of endometriosis is made by surgery. The definitive diagnosis of endometriosis can be made by pathological examination of the biopsy taken from the endometriosis focus that appear brown-black in the form of gunpowder burns in the abdominal cavity, on the uterus or in the ovary during surgery. It is not right to do surgery just to make a diagnosis. In which cases chocolate cyst should be operated, you can find out later in the article.
Endometriosis staging can only be done with surgery. During chocolate cyst surgery, laparoscopic, that is, closed method, is scored by looking at the location, width and depth of the endometriosis and the stage of the disease is tried to be determined. The stage of the disease is not directly proportional to pain, dyspareunia (painful sexual intercourse) and infertility. In other words, while the disease stage is low, complaints and symptoms may be high.
American society of reproductive medicine staging;
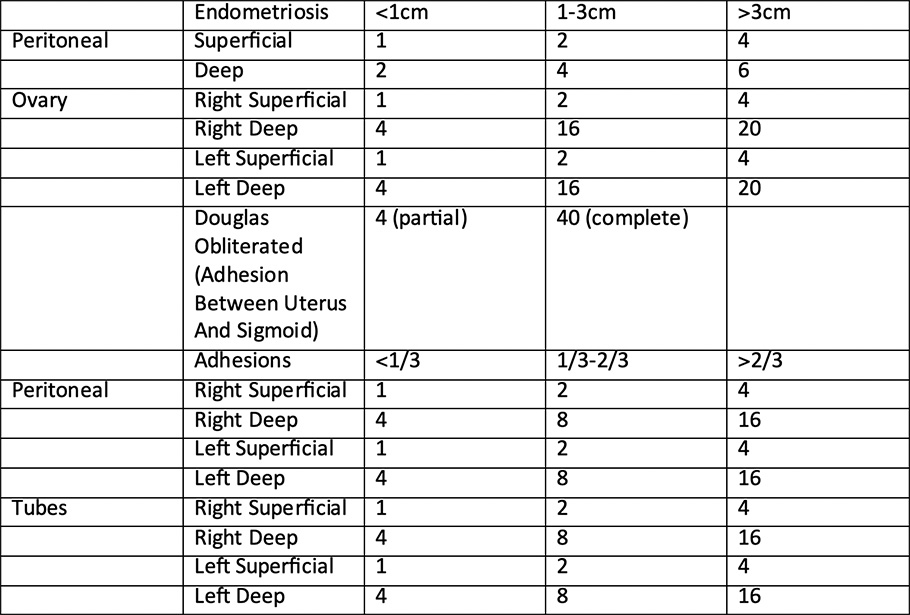
According to this scoring;
Chocolate cyst treatment is determined by whether the patient wants a child, the stage of the disease, its symptoms and age. There are 5 options for chocolate cyst treatment.
This treatment approach is carried out in patients who do not have any complaints, with close follow-up of the cyst. Since there are not many complaints in chocolate cysts, especially in the first stages, the cyst can be surgically removed and the ovarian reserve of the woman can be prevented from being adversely affected.
In this treatment, the patient's pain is tried to be reduced. Excessive prostaglandin production in the physiopathology of endometriosis is tried to be prevented with non-steroidal anti-inflammatory drugs. When pain medications recommended to reduce painful menstrual cramps are not helpful, other treatments are switched.
This treatment only reduces groin pain and menstrual pain. It will not help a patient who wishes to conceive a child.
Chocolate cyst is an estrogen dependent disease. Considering this logic, the idea has been put forward that treatments that lower body estrogen can regress or completely eliminate the disease. Studies have shown that hormonal drugs are beneficial in the treatment of chocolate cyst, and in practice these drugs are used in the treatment of endometriosis.
The aim of the hormonal treatment of chocolate cyst is to prevent the bleeding of the endometriotic tissue by preventing the hormonal stimulation in the menstrual cycle. However, it should be known that hormone therapy is only a suppressive treatment. If the hormone drug is stopped, the disease will recur. Therefore, hormonal drugs should be used for a long time.
It should also be known that pregnancy will not occur while using hormonal drugs. Patients using hormonal drugs should be informed that they cannot become pregnant during the treatment process.
The drugs used in the treatment of endometriosis can be summarized in 5 groups;
1. Birth control pills: Birth control pills are a good option in cases of mild endometriosis. It should be used for at least 6-12 months. Birth control pills are effective in reducing menstrual pain and in the progression of the disease. 3-month controls are appropriate during the drug use process.
2. Progesterone-containing drugs: Progestin-containing drugs are used in the treatment of endometriosis through the same mechanism as birth control pills. These drugs are taken by mouth daily. Progesterone injections made every 3 months can also be used in treatment. Hormone spiral reduces menstrual pain and chronic inguinal pain by 80%. Irregular spotting bleeding is one of the most common complaints in those who use these drugs.
3. Dan***: A derivative of nortesterone, dan*** has a progesterone-like effect. It lowers the level of estrogen in the body. The most important factor limiting the use of Dan*** is its side effects. Pimples (acne),lubrication on the skin, thickening of the voice, weight gain and edema are the obvious side effects.
4. Gona*** Releasing Hormone Analogs: This drug is administered once a month in the form of an injection. 2-3 of the treatment. There is a significant decrease in endometriosis complaints. Because this treatment creates a temporary menopause environment. However, this treatment should not be given longer than 6 months. Because gona*** releasing hormone analogues cause bone resorption.
5. Aromatase inhibitors: In addition to other treatments, aromatase inhibitors can also be given in the treatment of chocolate cyst.
Treatment of chocolate cyst with hormone drugs can only be applied to patients who do not want children. Because these drugs suppress ovulation and menstruation, the patient cannot become pregnant.
Hormones given externally in patients who are not considering children may be effective in reducing or eliminating the effects of endometriosis disease. Due to the increase and decrease in hormone levels in each monthly menstrual cycle, the endometrial tissue thickens, sheds and bleeds.
With hormonal drugs taken from outside, the growth of this tissue can be slowed down or new formations can be prevented. However, this approach in the treatment of chocolate cysts is not a permanent solution for patients. Because after the discontinuation of hormone therapy, the discomfort in patients begins to recur.
Surgery is the most appropriate treatment option for those who want a child or have severe endometriosis. In the surgical treatment of endometriosis, it is aimed to remove or destroy all endometriotic foci, to remove all adhesions and to optimize the pelvic (hip bone internal organs) anatomy as much as possible.
If there is chocolate cyst symptoms at an advanced age and a family history of cancer and it is not desired to have a child again, the uterus and ovaries can be removed. The definitive treatment for endometriosis is removal of the uterus and ovaries.
If hormone replacement therapy is to be given after endometriosis surgery, progesterone therapy should be given along with estrogen. Because, if progesterone is not given, the disease may recur.
Endometriosis surgery is performed on patients who want a child and have advanced endometriosis symptoms.
Drugs used in the treatment of chocolate cyst with drugs prevent the patient from getting pregnant.
For this reason, patients with endometriosis symptoms and wanting a child should be treated with surgery instead of drug therapy. Studies have shown that after chocolate cyst surgery, symptoms are reduced and getting pregnant becomes easier. After the removal of the tubes for the problems caused by endometriosis in the tubes, the success of IVF treatment increases.
In patients who do not want children, drug treatment is tried first. In cases where there is no response to drug therapy, all endometriotic focus must be surgically removed.
Not every endometriosis needs surgery. If the chocolate cyst symptoms impair the patient's quality of life, the patient's complaints do not resolve despite drug treatment, the patient has a desire to have a child or if there is an emergency indication for surgery such as bursting (cyst rupture) or turning the cyst around itself (torsion),the chocolate cyst should be operated on.
In other cases, cyst treatment or follow-up treatment can be performed with medication.
This treatment can be applied for patients with severe pain complaints or chocolate cysts that exceed 4 cm in size. For the application of this method, the age of the patient, whether he wants a child, the severity of his complaints and the condition of the cyst are taken into account.
Endometriosis cyst surgery methods are of 2 types.
Open endometriosis cyst surgery is performed under general anesthesia or epidural anesthesia. The abdomen is entered through a pfannenstiel (groin) incision like a caesarean section. The foci of endometriosis in the abdomen, uterus and ovaries are removed one by one and burned.
If endometriosis is present, as much of the capsule as possible is removed, including the capsule, if possible without bursting it. At a certain stage towards the end of the procedure, the cyst ruptures because the base of the cyst, where it attaches to the ovary, is fused with the ovary.
If the endometriosis bursts, care is taken to prevent the disease from spreading and to prevent serious adhesions after surgery. Therefore, care must be taken to open the cyst late and in a controlled manner. If the chocolate cyst bursts uncontrollably, the abdomen should be washed thoroughly at the end of the operation.
In open endometriosis cyst surgery, in addition to the removal of endometriotic foci, adhesions in the abdomen should also be opened and normal anatomy should be ensured. After the abdomen is thoroughly washed, the folds are closed in anatomical plan. In open surgery, it has been observed that the chocolate cyst spreads to the skin and subcutaneous tissue. Therefore, extra care should be taken to prevent the spread of endometriosis tissue with surgical instruments or suture material.
Laparoscopic endometriosis cyst surgery is the gold standard surgical approach in the treatment of chocolate cysts in the current medical approach. Closed chocolate cyst surgery is the surgery to be preferred in terms of patient comfort and surgical success.
Closed endometriosis cyst surgery is performed under general anesthesia. Closed (laparoscopic) chocolate cyst surgery is performed by opening 0.5-1 cm 3-4 holes from the navel and groin area. Closed chocolate cyst surgery is performed with a laparoscopy camera with 20 times magnification and by creating an air chamber in the abdomen with CO2 gas. In this way, the surgical field is more clearly visible, adhesions are more easily separated, and less damage is done to the ovarian tissue.
The aim of closed chocolate cyst surgery is the same as open chocolate cyst surgery. Endometriosis foci in the abdomen, uterus and ovaries are removed and burned one by one. Intra-abdominal adhesions are removed. If there is a chocolate cyst, it is removed together with the cyst capsule. If the cyst leaks, the procedure is terminated after the abdomen is thoroughly washed with saline.
Endometriosis reduces ovarian reserve (ovarian reserve). If the tissues are treated carelessly during surgery, if too much electro cautery (electrical burning) is used, the ovarian reserve may decrease even more.
Especially in patients who want to have children, open or closed chocolate cyst surgery should avoid procedures that may decrease the ovarian reserve. Care should be taken to use atraumatic methods as much as possible. Bleeding should be controlled with laparoscopic sutures instead of the burning method.
In laparoscopic endometriosis surgery, deep endometriosis in the rectovaginal septum area, the area between the back of the uterus and the large intestine, may be missed. If this area is not completely cleaned, the patient's pain does not go away after surgery. For this reason, these areas should be carefully examined during laparoscopic chocolate cyst surgery.
The functionality of the ovaries and tubes can also be evaluated during closed endometriosis surgery. By administering methylene blue through the cervix, laparoscopic chocolate cyst surgery can determine whether the tubes are open or not. If the tubes are open, there will be 40-50% pregnancy within 3 months after the operation.
If hydrosalpenx has formed in the tubes due to adhesions due to endometriosis, the damaged tube should also be removed during closed chocolate cyst surgery. Because even if IVF is performed, the toxic fluid in the hydrosalpinx will flow into the inner cavity of the uterus and decrease the chance of the baby attaching to the uterus and pregnancy. Therefore, it would be the most rational way to remove the tube with hydrosalpinx along with the chocolate cyst.
If the tubes are closed or have lost their function in the patient who has undergone endometriosis surgery, if the woman is of advanced age, if she has been receiving pregnancy treatment for many years but cannot conceive, it is appropriate to start IVF treatment after 2 months of hormonal suppression because the chance of pregnancy naturally will be low.
There are many factors that affect the duration of chocolate cyst surgery. The most important factor affecting the duration of surgery is the experience of the surgeon and the prevalence of the disease. The more common the disease and the more adhesions, the longer the surgery will take.
The surgeon's mastery of anatomy and surgical technique also affects the operation time. The experience of the team in closed laparoscopic surgeries and the prevalence of endometriosis disease in the environment and intestines can affect the duration of surgery.
In addition, the selection and quality of the instruments used in closed chocolate cyst surgery as the correct gripping tips, their problem-free operation and the experience of the physician assistant also affect the duration of chocolate cyst surgery.
Considering these factors, chocolate cyst surgery takes between 45 minutes and 2 hours on average. Sometimes it can be seen that widespread deep endometriosis cases can last up to 4 hours.
Like any operation, chocolate cyst surgery has its risks. In fact, chocolate cyst surgery may be riskier than other gynecologic surgeries. Because endometriosis is a disease characterized by intra-abdominal adhesions and disruption of normal anatomy.
Most complications occur when these adhesions are opened and normal anatomy is created. The most important factor in reducing these complications is the experience and care of the surgeon.
An experienced surgeon is a surgeon who better predicts what can happen as a result of an action and has a better command of anatomical structures. However, complications may develop despite experience and careful behavior.
Because endometriosis surgery can be much more complicated than cancer surgery. Due to the possibility of endometriosis affecting anatomical structures such as the intestine, bladder and ureter, it may be appropriate to expand the surgical team with a colorectal surgeon and urologist if necessary.
The risks of chocolate cyst surgery can be summarized as follows.
Although the most effective treatment of chocolate cyst is surgery, chocolate cyst may recur after this surgery. Because surgery is a suppression treatment just like hormone therapy, it does not completely eliminate the disease. In 30% of patients, chocolate cyst recurs within 5 years.
The risk of recurrence of chocolate cysts should be discussed with patients before and after surgery and necessary precautions should be taken. If follow-up with hormonal treatment is continued after surgery, the recurrence rate within 5 years decreases to 5%.
Non-surgical treatment of chocolate cysts is possible to a certain extent with hormonal drugs and painkillers. Especially in women who do not want to have children, hormone therapy can be performed. However, both surgery and hormone therapy are suppressive treatments. This means that endometriosis may recur after surgery or when hormone therapy is stopped.
Unless the genetic predisposition and other mechanisms underlying chocolate cysts are eliminated, a definitive treatment of the disease is not possible. A permanent cure for endometriosis, the mechanism of which is not even fully understood, is not yet known. However, genetic studies on chocolate cysts are still ongoing.
In patients who are nearing the end of their reproductive period and who have undergone repeated endometriosis surgeries, removal of the ovary and uterus may end the disease.
There are many factors that determine the price of chocolate cyst surgery. One of the most important factors affecting the price of surgery is the prevalence of endometriosis. The larger the chocolate cyst or the more common endometriosis is, the higher the chocolate cyst surgery prices will be.
If the patient has had endometriosis surgery before and now needs it again, the price of chocolate cyst surgery will be higher. Because each previous surgery increases the risk of surgery. This will increase the price of endometriosis surgery.
Another factor affecting chocolate cyst surgery prices is how the surgery will be performed. Open chocolate cyst surgery prices are cheaper than laparoscopic chocolate cyst prices. This is because the materials and surgical equipment used in laparoscopic chocolate cyst surgery are more costly and expensive. This increases the prices of closed chocolate cyst surgery.
Another factor that determines chocolate cyst surgery prices is the hospitals where the surgery will be performed. While there is no charge in public hospitals, the fees to be charged in private hospitals vary according to the group of the hospital.
The best doctor to perform chocolate cyst surgery is the one with the most surgical experience and who has established an endometriosis surgical team. Chocolate cyst surgery is not a simple operation, it can be as complicated as cancer surgery. For this reason, the best doctor who performs chocolate cyst surgery is the doctor who has seen and operated the most endometriosis patients.
The treatment of endometriosis patients encountered at different stages is individualized. If the prevalence of the disease is suspected, colonoscopy and kidney ultrasound may be requested before surgery. The bladder and ureter are examined for endometriosis nodules.
You can learn about the best endometriosis surgeon from the references of patients who have undergone surgery, and you can research postoperative ovarian preservation and conception rates. You can get advice from doctors who specialize in surgery on this subject.
Cysts have a 4 percent chance of carrying malignant and cancer-causing cells. Ovaries that look like endometrioma may contain endometrioid or clear cell type tumors at very rare rates.
This question is one of the most curious questions of patients. Chocolate cyst can prevent pregnancy by reducing ovarian reserve or disrupting pelvic anatomy, causing obstruction in the tubes. However, there are many women with chocolate cysts who become pregnant on their own. Therefore, although it cannot be said that the presence of a chocolate cyst in the ovary alone definitely prevents pregnancy, it has been shown by scientific studies that it reduces fertility. One of the most important factors determining the relationship between chocolate cysts and infertility is the prevalence (stage) of endometriosis. The more advanced the disease is, the more likely infertility is.
Chocolate cyst pain occurs during menstruation in the form of groin pain, low back pain, abdominal pain, pain in the leg. These pains occur especially during menstruation or in the premenstrual period, and the pain goes away after menstruation is over. Interestingly, pain and the stage of the disease are not always directly proportional.
If there is bowel involvement, pain may be felt during defecation. If there is bladder involvement, it may cause pain, aching or bleeding during urination.
The likelihood of a chocolate cyst in menopause is very low. This is because chocolate cyst is an estrogen-dependent disease and as estrogen levels decrease during menopause, the chocolate cyst shrinks or disappears completely.
If the chocolate cyst does not shrink or grow in menopause, closed chocolate cyst surgery is necessary to eliminate the risk of cancer and to make a pathological diagnosis. And the material taken must be sent to pathology to determine whether it is cancerous or not.
Chocolate cyst discharge can be brown, mud-colored. Chocolate cyst discharge may be in the form of brown discharge before or after menstruation. Chocolate cyst may also cause discharge.
If the chocolate cyst affects the gastrointestinal system, it may cause indigestion, bloating and nausea. Nausea and gas complaints increase especially before menstruation and decrease after menstruation ends.
Chocolate cyst does not bleed during pregnancy. However, the chocolate cyst may burst or the ovary may turn around and cause torsion. It can cause a pelvic abscess called inguinal abscess. In these cases, the cyst may need to be removed by emergency surgery, even if there is a pregnancy.
Although it is not known for certain, the reason why the endometrium tissue is located in an area other than the uterus (ovary, the inner membrane of the abdominal cavity, the surface of the outer wall of the uterus) is listed as bleeding from the tubes back into the abdominal cavity during menstruation, immune system factors of the fluids in the intra-abdominal cavity, genetic factors.
Chocolate cysts are cysts formed when the glandular tissue in the endometrium settles on the ovarian surface and the bleeding into the capsule formed by the superficial collapse is collected in the ovaries. The color of the fluid collected in the cystic structure is pending blood and is popularly called chocolate cyst because of its dark brown color and appearance resembling melted chocolate.
In this type of patient group, the best treatment approach would be to keep the cyst under observation for a certain period of time without resorting to surgical intervention. If there is an elevated Ca125 value, which is a tumor marker in blood tests, or if the diameter of the chocolate cyst exceeds 4-5 cm, surgical intervention may be decided in patients.
Prior to laparoscopic surgery, the ovarian reserve capacity of the patient should be evaluated by counting the ovarian sacs by ultrasound and measuring AMH (antimüllerian hormone). If it is determined that the woman's ovarian capacity is low as a result of this evaluation and if the woman is childless, the surgical intervention should be avoided as much as possible.
In patients with low ovarian reserve, we may recommend direct in vitro fertilization if they want to have children. In patients in this situation, Ca125 measurements should be performed at 3-6 month intervals. In women who have children or who do not want to have children in the future, laparoscopic surgical removal of the cyst should be performed.
In these patients, ovarian reserve should be evaluated first. If it is determined that this reserve is sufficient, if the cyst is unilateral, laparoscopic surgery and the tubes are healthy, the woman should be expected to conceive spontaneously for 6-12 months depending on the woman's age.
In women with poor ovarian reserve, especially in women over 38 years of age or if the cyst is bilateral, the best treatment approach is direct IVF treatment. It is recommended not to enter the cyst during egg collection during IVF treatment. If this is not observed, i.e. if a needle is inserted into the cyst, there may be an increased risk of groin infection (pelvic infection and abscess) and ovarian abscess.
There is no consensus on which treatment methods should be applied to women with chocolate cysts who have repeated failures in IVF treatment.
Surgical removal of the chocolate cyst may be recommended for women with three or more failures in IVF. In this group of patients, spontaneous pregnancy has been achieved in 50% of cases after laparoscopy.
Complications of laparoscopic surgery are high in such patient groups. If the patient does not complain of pain, then close follow-up is recommended. In women who do not want to have children and complain of pain, the uterus and ovaries may be removed.
If patients want to have children, in vitro fertilization treatment can be applied. However, the tubes of the patients should be evaluated before this treatment. Because there may be adhesions that may occur after repeated surgical interventions and blockage in the tubes after the tubes are affected by endometriosis.
The tubes may have a sausage-like appearance and may be filled with endometriosis tissue. This factor can reduce the woman's chances of pregnancy even with IVF. When a blockage in the tubes is detected, it may need to be removed laparoscopically or closed in the area adjacent to the uterus.
If laparoscopy carries a high risk for patients, then hysteroscopic sterilization techniques can be used.
In our patients who come for recurrent endometriosis surgery, we often encounter a frozen pelvis structure in which all organs in the groin area (bladder, intestines, uterus and ovaries) adhere to each other. In such cases, the approach of the Endometriosis surgery team reduces complication rates.
The endometriosis surgical team consists of an endometriosis surgeon, gynecologist, colorectal (bowel) surgeon and urologist. The whole team should have a high level of experience in laparoscopic approach.
Adenomyosis is when the endometriosis tissue that forms the inner wall of the uterus is located in the muscle tissue of the uterus. It gives symptoms by bleeding into the muscle tissue during each menstrual period. It becomes more frequent with increasing female age. Adenomyosis can be focal, i.e. located in one area of the uterus, or diffuse, i.e. diffusely involving the uterus.
Adenomyosis adheres to the uterine wall in a radial way and it is very difficult to separate from the uterine myometrium tissue because it is not encapsulated like fibroids. On ultrasound examination, it can be compared with the appearance of fibroids in the uterus.
The most important symptom of adenomyosis is severe menstrual and non-menstrual groin pain. Bleeding irregularities, prolonged bleeding and difficulty in conception may also be experienced. There may be complaints of pain during sexual intercourse. Sometimes adenomyosis can develop without any symptoms. Adenomyosis can sometimes give similar symptoms and be confused with fibroids.
Hormones and painkillers used in the treatment of chocolate cysts can be used in the treatment of adenomyosis. Hormonal spirals are also effective in the treatment of adenomyosis. Hormone medication or hormonal spiral is useful in reducing the amount of bleeding and pain
Surgical alternative may be considered in patients who do not respond to medication or hormonal spiral. Laparoscopic surgery is recommended for focal adenomyosis in the uterus, while open surgery is preferred in cases of widespread adenomyosis in the uterus.
The uterus can be removed in women at the end of reproductive age. Patients who have difficulty conceiving may be offered IVF treatment before surgery.
If endometriosis surgery is performed laparoscopically, the patient can stand up within 4-6 hours and be discharged within 24 hours after surgery. These patients can return to daily life or work in 1 week. If open surgery is performed, hospitalization may take 2 days and return to work may take up to 2 weeks.
In endometriosis surgery, if repair of the intestinal wall has been performed, it is recommended that the patient be monitored in the hospital for 5 to 7 days for intestinal leakage control.
If ureter or bladder repair is performed in endometriosis surgery, the patient can be discharged with a bladder catheter or ureter catheter after urine leakage control with postoperative imaging techniques. The bladder catheter is removed after 1 week and the ureter catheter after 3 or 6 months.
In endometriosis surgery, if a certain part of the intestine is removed (segmental resection) and end-to-end joining is performed, an ileostomy (opening of the intestine into the abdomen) can be opened to the patient as a protective measure. This is preferred if the level of the intestine area joined to the end is close to the anus.
In this method, which reduces the risk of leakage and increases patient safety, defecation is performed through the ileostomy bag attached to the abdominal wall. After 3 months, the intestinal segment in the abdominal wall is taken into the abdomen with the surgery to be performed and the intestinal segment that is joined end-to-end and healed starts to work.
Pregnancy plan after chocolate cyst surgery is made according to the findings obtained during surgery. If the tubes are found to be in good condition and the patient is not of advanced age, natural pregnancy can be tried for 3 to 6 months 2 months after the operation. If the condition of the tubes in chocolate cyst surgery is unhealthy or if the tubes need to be removed, IVF treatment can be applied 2 months after surgery.
After pregnancy occurs, a negative development in the pregnancy process is rare. Acute abdominal pain caused by leaks from chocolate cysts may be encountered rarely.
There is no restriction on sexuality after chocolate cyst surgery. The patient can have sexual intercourse when her general condition improves after surgery. Since different pain thresholds of patients play a role in this period, no exact time is given.
Chocolate cyst disease can be suppressed with medication and the complaints caused by the disease can be reduced. However, there is no definitive treatment for endometriosis with medication. The disease continues throughout the reproductive age with the support of the ovarian estrogen hormone.
In chocolate cyst disease, if there have been recurrent surgical processes and the patient has completed reproduction, the decision to remove the uterus and ovaries may be made. When making this decision, the risks of osteoporosis and cardiologic risks due to estrogen deficiency should be evaluated.
Endometriosis surgery is performed by an endometriosis surgery team specialized in closed surgery approach to chocolate cysts. The entire team should have a high level of experience in the laparoscopic approach.
The approach and surgical planning of the endometriosis surgery team reduces complication rates. The chocolate cyst surgery team includes a gynecologist, a colorectal surgeon and a urologist, led by an endometriosis surgeon.
The endometriosis surgery team consists of an endometriosis surgeon, gynecologist, colorectal surgeon and urologist who work together to evaluate the patient before surgery. The team may meet on certain days of the week to plan the approach to the patient.
The cohesion of the team members and the high number of operations performed annually reduce complication rates. The team members work full-time or part-time in the endometriosis center under the direction of the gynecologist endometriosis surgeon.
Ankara Endometriosis Surgery is performed by Prof. Dr. Önder Koç in the best equipped private hospitals.
Hello, my name is Sajedah. I am interested in Endometriosis excision surgery. It currently has my uterus and my ovaries stuck together and I would like a surgery to remove it. Is it possible to have an estimate? Thank you
Hello Sajedah. Get well soon we can help you our place is in Ankara Turkey you can contact us for this process 05052874333
